




Contents
Scroll to:
https://doi.org/10.25207/1608-6228-2024-31-4-17-29
Scroll to:
Background. Undifferentiated connective tissue disease is the subject of research in a large number of medical specialties, as it leads to an aggravated course of various diseases. In the presence of this pathology during pregnancy, the incidence of such complications as preeclampsia, gestational diabetes, and placental abruption increases. Failure to carry a pregnancy to term can be associated with various causes, including the activity of myocytes, while the pathology in question involves the connective tissue of the uterus. In this connection, it seems necessary to study the impact of undifferentiated connective tissue disease on pregnancy outcomes in order to administer timely treatment.
Objectives. To assess how undifferentiated connective tissue disease affects the risk of failure to carry a pregnancy to term.
Methods. An observational cohort prospective study was conducted among pregnant women who were under antenatal care in 2021–2022. The study was performed at the premises of the Clinical Maternity Hospital of Minsk Region (Republic of Belarus). The patients were divided into two groups: an exposed group comprising 59 patients with diagnosed undifferentiated connective tissue disease and a nonexposed group comprising 59 patients without this pathology. Both groups were divided into subgroups according to the obstetric outcome. The exposed group included a subgroup of 17 undifferentiated connective tissue disease patients who had failed to carry pregnancy to term (miscarriage and preterm labor) and a subgroup of 42 undifferentiated connective tissue disease patients with delivery at term. The nonexposed group included a subgroup of five women without undifferentiated connective tissue disease who had failed to carry pregnancy to term (miscarriage and preterm labor) and a subgroup of 54 women without undifferentiated connective tissue disease and with delivery at term. According to ICD-10, abortive outcomes occurred before 21 weeks and six days gestation; labor that occurred at 22–36 weeks and six days gestation was considered preterm, whereas in the case of delivery at term, the baby was born at 37–41 weeks and six days gestation. The obstetric, gynecological, and somatic history, as well as pregnancy outcomes, were analyzed. Statistical processing of data was performed using the following software: Statistica 12.0 (StatSoft, USA), Microsoft Excel 2016, Epi InfoTM 7.2.6.0 (USA), and MedCalc 15.8 (MedCalc Software, Belgium). In hypothesis testing, differences were considered statistically significant at p < 0.05.
Results. In the group of undifferentiated connective tissue disease patients, metrorrhagia was statistically significantly more common than in the patients without undifferentiated connective tissue disease: 18 out of 59 (30.5 %) and six out of 59 (10.2 %), respectively, p = 0.012. The obstetric history revealed no statistically significant intergroup differences, p > 0.05. In the undifferentiated connective tissue disease patients, the following diseases were statistically significantly more common: myopia, spinal scoliosis, lower limb varicose veins, chronic tonsillitis, mitral valve prolapse, and iron deficiency anemia (p < 0.05). The incidence of new cases of failure to carry a pregnancy to term in the cohort during the observation period amounted to 18.6 % for the patients in both groups. The pregnancy ended prematurely in 17 out of the 59 undifferentiated connective tissue disease patients (28.8 %) and in five out of the 59 patients without undifferentiated connective tissue disease (8.5 %), relative risk of 3.4 (95 % CI:1.3–8.6), p = 0.005.
Conclusion. Undifferentiated connective tissue disease increases the risk of failure to carry a pregnancy to term by 3.4 times. Timely diagnosis and treatment of undifferentiated connective tissue disease at the stage of preconception preparation can reduce the incidence of failure to carry a pregnancy to term.
Grudnitskaya E.N., Nebyshynets L.M. Pregnancy outcomes in patients with undifferentiated connective tissue disease: An observational cohort prospective study. Kuban Scientific Medical Bulletin. 2024;31(4):17-29. https://doi.org/10.25207/1608-6228-2024-31-4-17-29
One of the important aspects of demographic policy is female reproductive health, as well as a reduction in maternal and infant morbidity and mortality. Failure to carry a pregnancy to term is regarded as a serious medical and social problem since it can undermine female reproductive health, as well as increase morbidity and mortality among newborns. Prevention of miscarriage and preterm labor is one potential way to increase the birth rate. Modern safe motherhood practices offer a comprehensive approach to prenatal care, optimal delivery, as well as early detection and timely correction of gynecological and extragenital diseases. Despite the availability of methods for correcting complications during pregnancy, extragenital diseases still constitute a significant factor affecting maternal and fetal health.
In recent years, special attention has been given to hereditary connective tissue disorders, which constitute a significant medical and social problem. Among hereditary connective tissue disorders, two groups can be distinguished: monogenic forms with well-defined diagnostic criteria and multifactorial nonsyndromic forms for which no definitive molecular confirmation is currently available. These forms — referred to as undifferentiated connective tissue disease (UCTD)—are caused by genetic mutations and manifest themselves in the progressive disruption of connective tissue structure and function in various organs and systems. The realization of genetic defects in UCTD depends on the transient expression of mutated genes and external conditions [1]. UCTD is commonly diagnosed when a combination of phenotypic features is present that are not consistent with any of the differentiated forms of connective tissue disease1 [2].
The number of UCTD signs in children is minimal [1][3]. Adolescence is marked by an increase in height, body weight, and, consequently, connective tissue. This period is considered critical, as starting from it, the number of signs increases, and by the age of 40 years, symptoms manifest themselves in the vast majority (80 %) of patients if the prerequisites exist (genetic defects and malnutrition) [2]. Sex also plays a role. Studies show that women are more susceptible to UCTD than men. This fact can be attributed to the hormonal status in women, which affects the strength and elasticity of connective tissue. Some phenotypic features of UCTD are found in first-degree relatives on the mother’s side (mother and sister) in 93.4 and 84.6 % of cases, respectively [4].
In the population, the prevalence of UCTD reaches 20 %.2 No accurate data on the prevalence of UCTD among women of reproductive age are available; this pathology is reported by different authors with a frequency ranging from 20–30 % [5] to 60–80 % [6]. Depending on the involvement of body systems in the pathologic process, the main clinical symptoms may include diseases of the heart, kidneys, vessels, joints, and spine, as well as complications of pregnancy and labor [7]. Connective tissue is also present in the reproductive system, which is inevitably affected in the presence of UCTD. It is known that women with UCTD exhibit a higher morbidity with chronic somatic pathology and lower reproductive health indicators as compared to women without UCTD [7]. The myometrium consists of smooth muscle cells; however, due to the presence of a large number of connective tissue partitions between muscle bundles and vessels, the percentage of myocytes in the uterus varies from 42 to 85 % [8]. The endometrial stroma is characterized by vascular impairment due to decreased formation of Type IV collagen, matrix metalloproteinase-9, and tissue inhibitor of metalloproteinases-1. This is a significant factor leading to the inconsistency between the endometrial structure and the menstrual cycle phase, which can complicate implantation, embryo invasion, chorion and placenta formation, resulting in failure to carry a pregnancy to term [9].
Dysplastic processes in connective tissue constitute a serious medical and social problem, which determines the need to study the pregnancy outcomes in patients with UCTD in order to medically prevent its complications.
The study aims to assess how UCTD affects the risk of failure to carry a pregnancy to term.
An observational cohort prospective study was conducted among 118 pregnant women under antenatal care with an obstetric outcome.
The study was conducted at the premises of the Clinical Maternity Hospital of Minsk Region (Republic of Belarus). Pregnancy outcomes, as well as external and/or visceral signs of connective tissue disease were evaluated in patients enrolled for antenatal care at the institution between January 01, 2021 to January 31, 2022.
Inclusion criteria
Singleton pregnancy; gestational age between eight and twelve weeks inclusive; age of women between 18 and 45 years; no restrictions on the number of pregnancies and births.
Exclusion criteria
Multiple pregnancy; pregnancy after assisted reproductive technology; recurrent miscarriage; history of miscarriage or premature labor; second and third trimesters of pregnancy; severe extragenital pathology; sexually transmitted infections; pregnant women infected with human immunodeficiency virus; refusal to sign informed consent.
Removal criteria
Diagnosed congenital fetal malformations and monogenic disruption of connective tissue structure and function; refusal to answer questions, be examined, or undergo an instrumental examination; factors that increased the risk for the patient, prevented the patient from fully complying with the conditions of the study, or prevented the patient from completing the study.
Description of the eligibility criteria (diagnostic criteria)
UCTD was diagnosed according to the clinical guidelines “Undifferentiated Connective Tissue Diseases” (2019).3 According to ICD-10, abortive outcomes occurred before 21 weeks and six days gestation; labor that occurred at 22–36 weeks and six days gestation was considered preterm, whereas in the case of delivery at term, the baby was born at 37–41 weeks and six days gestation.
Selection of group members
The study included 118 female patients who were divided into two groups. The main (exposed) group consisted of 59 patients with UCTD, while the comparison (nonexposed) group comprised 59 pregnant women without UCTD. Taking the obstetric outcome into account, the following subgroups were distinguished: UCTD patients who had failed to carry pregnancy to term (miscarriage and preterm labor) (n = 17); UCTD patients with delivery at term (n = 42); patients without UCTD who had failed to carry pregnancy to term (miscarriage and preterm labor) (n = 5); patients without UCTD and with delivery at term (n = 54).
Main parameters of the study
Differences in the obstetric, gynecologic, and somatic histories; pregnancy outcome; effect of UCTD on pregnancy outcomes in the study groups.
Additional parameters in the study
No additional parameters were analyzed in the study.
Methods for measuring the target parameters
Patients underwent clinical and instrumental examination, which included history taking and analysis of complaints, general medical and gynecological examination, and anthropometry, including measurement of body weight (kg), height, hand length, foot length, arm span, and upper and lower body segment length (cm) and BMI estimation (kg/m²), as well as analysis of pregnancy outcomes.
Variables (predictors, confounders, and effect modifiers)
Factors that could skew the results were initially classified as exclusion criteria and were not observed in the studied patients.
Principles behind sample size determination
Epi InfoTM software (available at: http://www.cdc.gov/epiinfo/) was used to estimate the cohort size. The following parameters were used for data entry: confidence interval — 95 %; power of the study — 80 %; size ratio of nonexposed to exposed groups in the cohort — 1; event rate in the nonexposed group — 25 %; odds ratio — 2. According to the Kelsey’s formula, the size of the “exposed” and “nonexposed” samples amounted to 59 people each, i.e., a total of 118. An 80 % “response” was predicted, given dropout from the study, so the sample was increased by 20 %. The final cohort size amounted to 142 patients.
Statistical methods
Data were statistically processed using the following software: Statistica 12.0 (StatSoft, USA), Microsoft Excel 2016, Epi InfoTM 7.2.6.0 (USA), and MedCalc 15.8 (MedCalc Software, Belgium). The normality of quantitative indicators was checked using the Shapiro—Wilk test. For normal distribution of quantitative indicators, data are given as mean (M) with standard deviation (SD); for distribution other than normal, data are presented as median (Me) with interquartile range (Q1; Q3); qualitative indicators are presented as frequency or proportion in the group ( %).The distribution of most characteristics does not follow the normal distribution, so the quantitative data of two independent groups were compared using a nonparametric statistical analysis method: the Mann—Whitney test. In terms of category characteristics, the groups were compared pairwise using the two-tailed Fisher’s exact test since in many comparisons, the proportion of table cells with expected observations of less than 5 exceeded 20 %. The odds ratio (OR) and its statistical significance were estimated using a 95 % confidence interval (CI). In hypothesis testing, differences were considered statistically significant at p < 0.05.
The sampling was carried out via the continuous sampling method. The phenotypic features of UCTD were assessed in all study participants. The groups were formed according to the presence or absence of UCTD. The exposed group included women with UCTD whereas the unexposed group included women without UCTD. Depending on the pregnancy outcome—failure to carry a pregnancy to term or delivery at term—each group was divided into two subgroups.
The study included 142 pregnant women who sought antenatal care. All women were evaluated and were found to meet the inclusion criteria of the study: singleton pregnancy; gestational age between eight and twelve weeks inclusive; age of women between 18 and 45 years. During observation, 20 women were removed from the study. Congenital fetal malformations were diagnosed in four pregnant women during prenatal screening, and 16 pregnant women refused to answer questions, be examined, or undergo an instrumental examination. Also, four women dropped out of the observational study due to a change of residence. A total of 118 pregnant women completed the study. An analysis of data on obstetric, gynecological, and somatic pathologies, as well as the phenotypic features of UCTD, provided a means to distinguish two groups of pregnant women: those with UCTD, i.e., the exposed group (59 women), and those without UCTD, i.e., the nonexposed group (59 women). After assessing the obstetric outcome, the groups were divided into subgroups. The subgroup of UCTD patients who had failed to carry pregnancy to term included 17 patients, and the subgroup with UCTD and delivery at term included 42 women. The subgroup of patients without UCTD who had failed to carry pregnancy to term included five patients, while the subgroup without UCTD and delivery at term included 54 women (Figure).
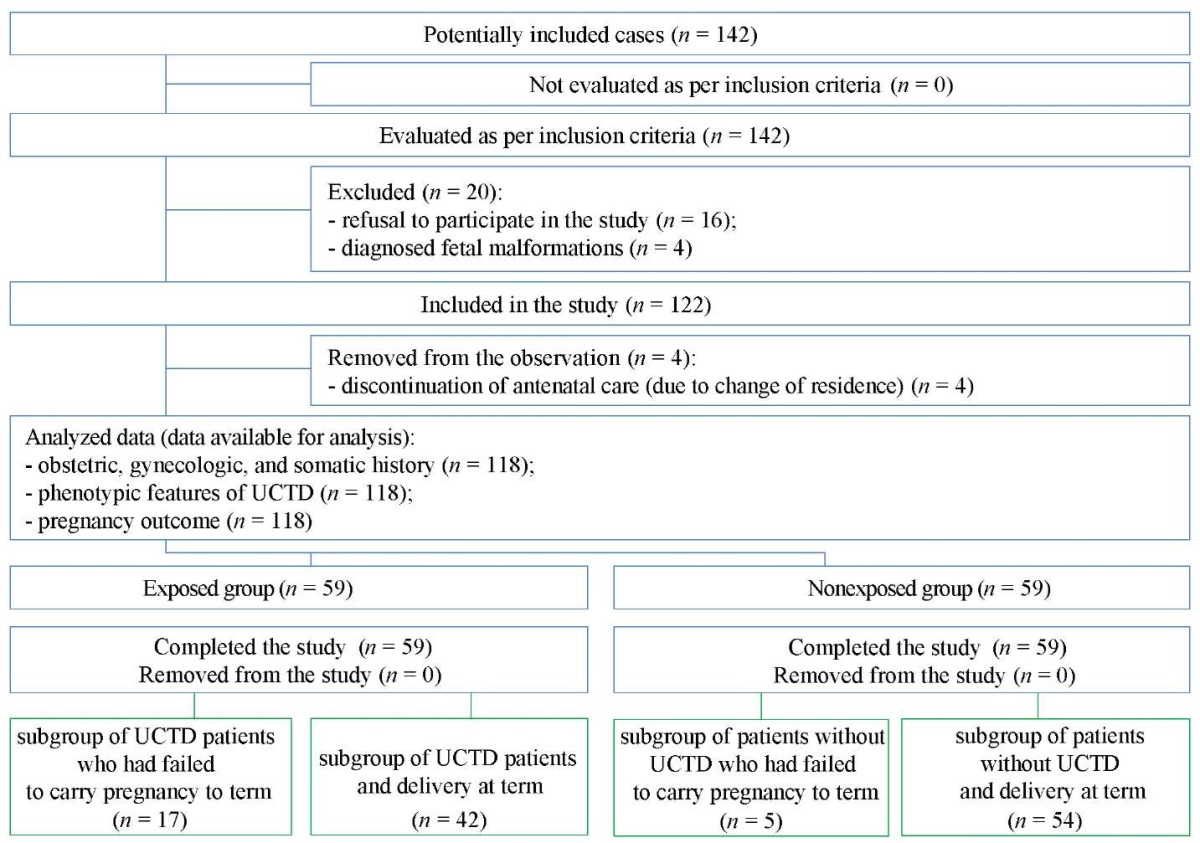
Fig. Block diagram of the study design
Note: The block diagram was created by the authors (as per STROBE recommendations).
Abbreviation: UCTD — undifferentiated connective tissue disease.
Рис. Блок схема дизайна исследования
Примечание: блок-схема выполнена авторами (согласно рекомендациям STROBE).
Сокращение: UCTD — недифференцированная дисплазия соединительной ткани.
The study included a total of 118 women aged between 22 and 38 years, with a mean age of 32.1 ± 3.9 years. The mean age of women with UCTD was 31.5 ± 4.2 years while that of patients without UCTD was 32.6 ± 3.5 years (p > 0.05). The patients in the compared groups did not differ in terms of weight and height data: the height and weight of women were 168 (164; 172) cm and 63 (56; 75) kg in the exposed group and 165 (162; 170) cm and 58 (54; 70) kg in the nonexposed group, respectively (p > 0.05). The values of body mass index were consistent with the norm in both groups; however, in the group of UCTD patients, the body mass index was 22.3 (20.2; 26.5) (kg/m²), and in the group of women without UCTD, the index was 21.4 (19.5; 24.4) (kg/m²) (p > 0.05). Intergroup comparisons revealed no statistical weight and height differences (Table 1).
Table 1. Age, weight, and height data in the studied groups
Таблица 1. Возраст и весоростовые показатели в исследуемых группах
|
Parameter |
Exposed group (n = 59) |
Nonexposed group (n = 59) |
Significance level, p** |
|
Age (years), M ± SD |
31.5 ± 4.2 |
32.6 ± 3.5 |
0.93 |
|
Height* (cm), Me (Q1; Q3) |
168 (164; 172) |
165 (162;170) |
1.00 |
|
Body weight prior to pregnancy*, Me (Q1; Q3) |
63 (56; 75) |
58 (54; 70) |
1.00 |
|
Body mass index*(kg/m²), Ме (Q1; Q3) |
22.3 (20.2; 26.5) |
21.4 (19.5; 24.4) |
1.00 |
Note: The table was compiled by the authors;
* — median (interquartile range);
** — significance of differences was determined as per the Mann–Whitney test.
Abbreviation: Me — median.
Примечание: таблица составлена авторами;
* — медиана (интерквартильный интервал);
** — значимость различий определена согласно тесту Манна — Уитни.
Сокращение: Ме — медиана.
An analysis of gynecologic history in the studied groups found that in the UCTD group, the first menstruation occurred at the age of 13.0 ± 1.6 years, while in the group of patients without UCTD, the first menstruation was at the age of 13.4 ± 1.4 years (p > 0.05). Most women in the exposed and nonexposed groups had a menstrual cycle lasting between 24 and 38 days—the proportion of such patients was the same, i.e., 93.2 % in both groups (55 out of 59) (p > 0.05). A short menstrual cycle was observed in one woman without UCTD (1.7 %); no UCTD patients with a short menstrual cycle were identified (0 %), (p > 0.05). A long menstrual cycle (over 38 days) was observed in four out of the 59 exposed women (6.8 %) and in three out of the 59 (5.1 %) nonexposed women (p > 0.05). Also, the amount of menstrual blood loss in most women was consistent with the reference values: in 40 UCTD patients (67.8 %) and 53 patients without UCTD (89.8 %), p > 0.05.
In the exposed group, menorrhagia was statistically significantly more common than in the nonexposed group, i.e., in 18 (30.5 %) and six (10.2 %) women, respectively, p = 0.01. Scanty menstruation was noted in one woman with UCTD (1.7 %), while among women without UCTD, no scanty menstruation was observed (0 %), p > 0.05. In the exposed women, coitarche, on average, occurred at 19.0 ± 2.5 years, while in the nonexposed women, coitarche occurred a year earlier (at 18.1 ± 1.7 years). Also, although no statistically significant differences were found, the women without UCTD had more sexual partners than UCTD patients: 3 (2; 5) and 2 (1; 3), respectively (p > 0.05).
For the purpose of contraception, patients from both groups equally often used combined oral contraceptives—18 out of the 59 women (30.5 %) (p > 0.05). Most women from both groups preferred to use barrier methods: 31 UCTD patients (52.5 %) and 38 patients without UCTD (64.4 %) (p > 0.05). Intrauterine systems were used by two out of the 59 exposed women (3.4 %) and three out of the 59 nonexposed women (5.1 %) (p > 0.05). The use of the withdrawal method for the purpose of contraception was statistically significantly more common among the UCTD patients—eight women (13.6 %); patients without UCTD did not use this method (0 %), p = 0.01. No patients in the observed cohort reported combined use of contraceptive methods. Data on gynecologic history are presented in Table 2.
Table 2. Gynecologic history of the patients in the studied groups
Таблица 2. Гинекологический анамнез пациенток исследуемых групп
|
History |
Exposed group (n = 59) |
Nonexposed group (n = 59) |
Significance level, p *** |
|
Menarche* (years) |
13.0 ± 1.6 |
13.4 ± 1.4 |
0.54 |
|
Menstrual cycle (days) (% (abs.)) |
|||
|
<24** |
0 (0) |
1.7 (1) |
1.0 |
|
24–38** |
93.2 (55) |
93.2 (55) |
1.0 |
|
>38** |
6.8 (4) |
5.1 (3) |
1.0 |
|
Menstruation (amount) (% (abs.)) |
|||
|
Scanty (<10 mL/day)** |
1.7 (1) |
0 (0) |
1.0 |
|
Moderate (10–80 mL/day)** |
67.8 (40) |
89.8 (53) |
0.24 |
|
Heavy (>80 mL/day)** |
30.5 (18) |
10.2 (6) |
0.01 |
|
Contraceptive method (% (abs.)) |
|||
|
Barrier contraceptives** |
52.5 (31) |
64.4 (38) |
0.26 |
|
Combined oral contraceptives** |
30.5 (18) |
30.5 (18) |
1.0 |
|
Intrauterine contraceptives** |
3.4 (2) |
5.1 (3) |
1.0 |
|
Withdrawal method** |
13.6 (8) |
0 (0) |
0.01 |
|
Coitarche* (years) |
19.0 (2.5) |
18.1 (1.7) |
0.49 |
|
Number of sexual partners, Me (Q1; Q3) |
2 (1;3) |
3 (2;5) |
0.42 |
Note: The table was compiled by the authors;
* — Mean (standard deviation);
** — proportion of patients with the analyzed characteristic
(number of people with the analyzed characteristic);
*** — significance of differences was determined
as per the two-tailed Fisher’s exact test.
Примечание: таблица составлена авторами;
* — среднее (стандартное отклонение), Mean (standart deviation);
** — доля пациенток с анализируемым признаком
(количество индивидуумов с анализируемым признаком);
*** — значимость различий определена
согласно точному двустороннему критерию Фишера.
An analysis of obstetric history showed that in the UCTD group, the majority, i.e., 32 women (54.2 %), were primiparas, and 27 women (45.8 %) were secundiparas. In the group of patients without UCTD, most women were secundiparas, i.e., 35 out of the 59 women (59.3 %), with the number of primiparas amounting to 20 women (33.9 %), p > 0.05. No multiparas were found in the UCTD group (0 %), while the group of patients without UCTD included four women who had borne more than one child (6.8 %), (p > 0.05). The number of women who gave birth via cesarean section was higher in the exposed group than in the group of patients without UCTD, i.e., eight (13.6 %) and three (5.1 %) women, respectively, p > 0.05. No cases of preterm labor were found in the history of women included in the study. The nonexposed women underwent artificial abortion more often than the exposed women: 13 (22.0 %) and ten women (16.9 %), respectively, p > 0.05. No cases of miscarriage or recurrent miscarriage were reported in the history of women from the observed cohort. In preparation for the pregnancy, all observed patients from the cohort reported taking 400 mcg/day of folic acid and 200 mcg/day of potassium iodide orally for two months as part of the preconception preparation program. The obstetric history of women from both groups is presented in Table 3.
Table 3. Obstetric history of the patients from the studied groups
Таблица 3. Акушерский анамнез пациенток исследуемых групп
|
History |
Exposed group (n = 59) |
Nonexposed group (n = 59) |
Significance level, p ** |
|
Childbirth (% (abs.)) |
|||
|
Primipara* |
54.2 (32) |
33.9 (20) |
0.06 |
|
Secundipara* |
45.8 (27) |
59.3 (35) |
0.2 |
|
Multipara* |
0 (0) |
6.8 (4) |
0.06 |
|
Cesarean section* |
13.6 (8) |
5.1 (3) |
0.20 |
|
Abortions (% (abs.)) |
|||
|
Artificial abortion* |
16.9 (10) |
22.0 (13) |
0.64 |
Note: The table was compiled by the authors;
* — proportion of patients with the analyzed characteristic
(number of people with the analyzed characteristic);
** — significance of differences was determined
as per the two-tailed Fisher’s exact test.
Примечания: таблица составлена авторами;
* — доля пациенток с анализируемым признаком
(количество индивидуумов с анализируемым признаком);
** — значимость различий определена
согласно точному двустороннему критерию Фишера.
An analysis of somatic pathologies in the UCTD group revealed that the following diseases were statistically significantly more common: myopia — 35.6 % (21), spinal scoliosis — 30.5 % (18), lower limb varicose veins — 28.8 % (17), mitral valve prolapse (MVP) — 20.3 % (12), chronic tonsillitis — 23.7 % (14), and iron deficiency anemia — 15.3 % (9). The group of patients without UCTD included eight women with myopia (13.6 %), five women with spinal scoliosis (8.5 %), six women with lower limb varicose veins (10.2 %), three women with mitral valve prolapse (5.1 %), five women with chronic tonsillitis (8.5 %), and no women with iron deficiency anemia (0 %). For all intergroup comparisons, p < 0.05.
The somatic history of patients in both groups was comparable in terms of such diseases as nephroptosis (15 women (25.4 %) in the exposed group and eight women (13.6 %) in the nonexposed group) and folded gallbladder (18 women (30.5 %) in the exposed group and nine women (15.3 %) in the nonexposed group), p > 0.05. Hypothyroidism was more common in the nonexposed women—five women (8.5 %); in the exposed group, it was found only in three women (5.1 %), p > 0.05. Cases of arterial hypertension were found only in the UCTD patients— two women (3.4 %); no cases of arterial hypertension were found in the patients without UCTD (0 %), p > 0.05. Table 4 summarizes somatic diseases observed in the patients of the observed cohort.
Table 4. Proportion of patients with different diseases in the compared groups
Таблица 4. Доля пациенток с различными заболеваниями в сравниваемых группах
|
Disease |
Exposed group (n = 59) (% (abs.)) |
Nonexposed group (n = 59) (% (abs.)) |
Significance level, p |
|
Myopia* |
35.6 (21) |
13.6 (8) |
0.01# |
|
Chronic tonsillitis* |
23.7 (14) |
8.5 (5) |
0.04# |
|
Hypothyroidism* |
5.1 (3) |
8.5 (5) |
0.49** |
|
MVP* |
20.3 (12) |
5.1 (3) |
0.03** |
|
Folded gallbladder* |
30.5 (18) |
15.3 (9) |
0.08# |
|
Nephroptosis* |
25.4 (15) |
13.6 (8) |
0.16# |
|
Spinal scoliosis * |
30.5 (18) |
8.5 (5) |
0.01# |
|
Lower limb varicose veins* |
28.8 (17) |
10.2 (6) |
0.02# |
|
Arterial hypertension* |
3.4 (2) |
0 (0) |
0.248** |
|
Iron deficiency anemia* |
15.3 (9) |
0 (0) |
0.001** |
Note. The table was compiled by the authors;
* — proportion of patients with the analyzed characteristic
(number of people with the analyzed characteristic);
** — significance of differences was determined
as per the two-tailed Fisher’s exact test,
# — significance of differences was determined as per the chi-squared test.
Abbreviation: MVP — mitral valve prolapse.
Примечания: таблица составлена авторами;
* — доля пациенток с анализируемым признаком
(количество индивидуумов с анализируемым признаком);
** — значимость различий определена
согласно точному двустороннему критерию Фишера,
# — значимость различий определена согласно критерию хи-квадрат.
Сокращение: MVP — пролапс митрального клапана.
All patients in the exposed group were diagnosed with a comorbid somatic pathology. Dysplasticity manifests in various organs with the involvement of at least three body systems: visual, bronchopulmonary, endocrine, cardiovascular, gastrointestinal, urinary, and skeletal. Comorbidity of such diseases as myopia, spinal scoliosis, and lower limb varicose veins developing at a young age was predominant. This combination was found in 15 out of the 59 (25.4 %) patients. The second place was occupied by comorbidity of such diseases as iron deficiency anemia, nephroptosis, and MVP; this combination was found in seven out of the 59 women (11.9 %). No comorbid somatic pathology was found in the patients of the nonexposed group. Isolated cases of the following diseases were noted: myopia, chronic tonsillitis, hypothyroidism, MVP, folded gallbladder, nephroptosis, spinal scoliosis, and lower limb varicose veins. No morbidity with arterial hypertension and iron deficiency anemia was found in patients from the nonexposed group.
The UCTD patients had a more frequent family history of cancer—seven women (11.9 %)—as compared to those from the group of patients without UCTD—five women (8.5 %). However, the family history of patients without UCTD was more often burdened with type 1 and 2 diabetes mellitus: such cases were reported in the family history of six women (10.2 %) vs. four women (6.8 %) in the UCTD group. No patients from the nonexposed group had a family history of thromboembolic complications (0 %), whereas only one patient in the exposed group had a family history burdened with thromboembolic complications (1.7 %). All intergroup comparisons revealed no statistically significant differences (p > 0.05).
The conducted cohort study yielded the following results. A premature end of pregnancy (miscarriage and preterm labor) was statistically significantly more common in the group of UCTD patients than in the group of patients without UCTD, i.e., 17 (28.8 %) and five (8.5 %) women, respectively (p = 0.005).
The incidence of failure to carry a pregnancy to term in the cohort was calculated
Incidence in the observed cohort = (22 / 118) • 100 % = 18,6 %
For an analysis of the one-year cohort observational study, the data are presented in a fourfold table (Table 5).
In order to assess the relationship between UCTD and failure to carry a pregnancy to term, the odds ratio (OR) was calculated, and to assess the significance of the odds ratio, the limits of 95 % confidence interval (95 % CI) were determined: the identified relationship was considered statistically significant at p < 0.05 if the confidence interval did not include one. An analysis of the obtained data revealed that the risk of failure to carry a pregnancy to term was found to be 3.4 (95 % CI: 1.3–8.6) times higher in women with UCTD as compared to women without UCTD, p < 0.05.
Table 5. Incidence of new cases of failure to carry a pregnancy to term
(data are presented in absolute values)
Таблица 5. Частота новых случаев недонашивания беременности
(данные представлены в абсолютных величинах)
|
Groups |
Failure to carry a pregnancy to term (miscarriage and preterm labor) |
||
|
yes |
no |
Total |
|
|
With UCTD |
17 |
42 |
59 |
|
Without UCTD |
5 |
54 |
59 |
|
Total |
22 |
96 |
118 |
Note: The table was compiled by the authors.
Abbreviation: UCTD — undifferentiated connective tissue disease.
Примечание: таблица составлена авторами.
Сокращение: UCTD — недифференцированная дисплазия соединительной ткани.
No additional results were obtained during the study.
The study analyzed pregnancy outcomes in UCTD patients. It is shown that this pathology is associated with a high weight of miscarriages and preterm births. In the studied patient population, such diseases as myopia, lower limb varicose veins, MVP, spinal scoliosis, chronic tonsillitis, and iron deficiency anemia were statistically significantly more common (p < 0.05).
Not identified.
The favorable course of pregnancy and the newborn’s health directly depend on the physical status of the woman. In modern obstetrics, special attention is paid to UCTD since in women with this pathology, pregnancy is distinguished by several features that lead to various complications, including failure to carry a pregnancy to term. Pathological changes in UCTD are systemic in nature and accompanied by various clinical symptoms and manifestations: they reduce the quality of life, as well as negatively affecting fertility and the ability to work. A characteristic feature of UCTD is the minor manifestation of external signs, which often leads to their underestimation. The systemic insufficiency of connective tissue is involved in the pathologic development of reproductive organs, which may cause various obstetric complications. In UCTD, pathological processes result from changes in the connective tissue architecture caused by disturbances in the structural protein catabolism and/or anabolism of the connective tissue matrix, as well as changes in the activity of enzymes involved in these processes. Literature reports that women with UCTD have low body weight and suffer from malnutrition [9–11]. In the observed cohort, the height, weight, and BMI of women were consistent with the norm. Intergroup comparisons of these data for the exposed and nonexposed groups yielded no statistically significant differences. Both malnutrition and obesity in pregnant women statistically significantly increase the likelihood of adverse pregnancy outcomes [12–14]. In this study, the effect of excess weight or lack of it on pregnancy outcomes was excluded.
The reproductive disorder in UCTD may manifest itself since menarche. Frequent manifestations of the disorder include irregularities in the menstrual cycle and amount of menstruation. Dysplastic formation of structural elements of the stroma and vessels of the myometrium and endometrium is clinically manifested by variable menstrual cycle length, as well as painful and heavy menstruation. These processes result in the development of iron deficiency anemia. Hemostatic disorders in UCTD also include thrombocytopathies, decreased activity of clotting factors, which is clinically manifested in increased bleeding of the gums, nosebleeds, and formation of spontaneous hematomas on the body. An analysis of menstrual cycle length in the patients with UCTD showed no statistically significant differences as compared to the patients without UCTD. The UCTD patients were statistically significantly more common to suffer from menorrhagia and have a history of iron deficiency anemia. It is reported in the literature that people with UCTD have an increased risk of anemia, which should be taken into account in their medical care [15–19].
Rational contraceptive methods play an important role in preserving reproductive health. In spite of the current variety of contraceptive methods, over half of the women from both groups preferred to use barrier methods; combined oral contraceptives were used by one third of the women; intrauterine contraceptives were used by no more than 5 % of the examined women; only patients from the exposed group used the withdrawal method. The obtained data are consistent with the literature on women’s preference for contraceptive methods [20].
In the UCTD group, over half of the patients, i.e., 54.2 % (32 out of 59), were primiparas, less than half, i.e., 45.8 % (27 out of 59), were secundiparas, and no multiparas were present. The opposite data were obtained for the group of patients without UCTD: over half of the observed women, i.e., 59.3 % (35 out of 59), were secundiparas, while the number of primiparas was lower—33.9 % (20 out of 59); the group also included multiparas; however, they were the minority—6.8 % (four out of 59). The main cause of recurrent miscarriage in women with UCTD includes isthmicocervical insufficiency.
Undifferentiated connective tissue disease often causes obstetric complications in pregnant women: threatened premature end of pregnancy, late toxemia, and preterm labor. The combination therapy of threatened preterm labor in UCTD uses magnesium preparations that have proven efficacy. According to the literature, in order to reduce the risk of threatened miscarriage, risk of isthmicocervical insufficiency, and to increase the chances of carrying a pregnancy to term in patients with UCTD, a personalized preconception preparation is required: 400 mcg/day of folic acid; 200 mcg/day of potassium iodide orally for three months; 300 mg/day of Mg²+ preparations; 400 mg/day of glycine; multivitamin supplementation containing 10 mg/day of thiamine, 10 mg/day of riboflavin, 10 mg/day of pyridoxine, and 400 mg/day of tocopherol orally for three months [20]. All patients in the observed cohort took 400 mcg/day of folic acid and 200 mcg/day of potassium iodide orally for two months prior to delivery according to the clinical protocol.4
In UCTD, at least three body systems represented by no fewer than six signs are involved in the pathologic process.5,6 The phenotypic symptoms of UCTD are grouped depending on the involvement of organs and systems. The external and internal signs of UCTD are classified. The external signs are subdivided into bone, joint, and skin manifestations. The internal signs include dysplastic changes in the nervous system, visual system, cardiovascular system, respiratory system, urinary tract, and gastrointestinal tract, as well as hematopoietic, immune, and reproductive systems.
Such diseases as myopia, MVP, spinal scoliosis, lower limb varicose veins, and chronic tonsillitis were statistically significantly more common in the exposed patients. In the presence of vision disorder, patients complain of decreased visual acuity and headaches associated with prolonged eye strain. Myopia is the most common visual disorder manifestation in UCTD, accounting for up to 68 % [3]. In the observed cohort, myopia was statistically significantly more common in the UCTD patients than in the patients without UCTD, i.e., 35.6 % (21 out of 59) and 13.6 % (eight out of 59), respectively, p < 0.05.
Bone connective tissue disorders are associated with changes in and disruption of collagen structure, which is manifested by spinal scoliosis, kyphosis, and kyphoscoliosis. Eighteen of the 59 observed women with UCTD (30.5 %) had a history of spinal scoliosis, while the number of such women among patients without UCTD was statistically significantly lower—five out of the 59 women (8.5 %), p < 0.05. With the bone and joint system involved in the pathological process, the patients note night and morning pains in various parts of the spine, and increased pain with prolonged walking or from being in an uncomfortable position. Vertebral slippage (displacement of one vertebral body with respect to the adjacent vertebral body), osteochondrosis, and spinal scoliosis begin to develop in UCTD patients as early as in adolescence.7
In addition, UCTD in adolescence leads to the development of lower limb varicose veins [22], with its manifestations worsening during pregnancy and after childbirth, affecting the lesser pelvic area, perineum, and vulva [23]. In the medical history of the UCTD patients, varicose veins were found to be statistically significantly more common as compared to the group of patients without UCTD, i.e., 28.8 % (17 out of 59) and 10.2 % (six out of 59), respectively, p < 0.05.
In addition to maxillary sinusitis, sinusitis, frontal sinusitis, pharyngitis, and polyposis of maxillary sinuses, chronic tonsillitis is one of the manifestations of ENT disorder in UCTD [2]. This pathology was statistically significantly more common in the exposed patients than the nonexposed patients. Chronic tonsillitis was found in 23.7 % (14 out of 59) of the patients with UCTD and 8.5 % (five out of 59) of the patients without UCTD, p < 0.05.
The signs of UCTD involving the cardiovascular system include valve prolapse, aortic root dilation, atrial septal aneurysm, arterial aneurysms, as well as varicose veins of the lower limbs, vulva, and lesser pelvis, at a young age. The valve disorder can develop in UCTD patients as early as childhood, most commonly manifesting as Grade 1 or 2 MVP. The patients complain of palpitations, dyspnea, and increased fatigue. Complaints increase in times of increased physical and psycho-emotional stress, including during pregnancy, labor, and in the postpartum period [23][24]. In the observed group of women with UCTD, a history of MVP was statistically significantly more common than in the patients without UCTD: 20.3 % (12 out of 59) and 5.1 % (three out of 59), p<0.05.
Noteworthy is that despite the high prevalence of UCTD among women of reproductive age, it remains undetected by doctors of various specialties and is often diagnosed for the first time during pregnancy. The literature reports that UCTD is accompanied by the development of pregnancy complications: early toxemia, threatened miscarriage in the first trimester, threatened preterm labor, and uncompensated placental insufficiency [23][24]. The conducted cohort study revealed a statistically significant relationship between UCTD and premature end of pregnancy; the incidence of new cases of failure to carry a pregnancy to term during the observation period was 18.6 %, with an odds ratio (OR) of failure to carry a pregnancy to term of 3.4 in the presence of UCTD (95 % CI: 1.3–8.6).
Heavy menstruation and metrorrhagia are statistically significantly more common (p = 0.01) in women with UCTD as compared to women without this pathology, which should be taken into account when examining and providing them with medical care. In addition, high morbidity with somatic diseases was found in the exposed patients, among which iron deficiency anemia, myopia, MVP, spinal scoliosis, lower limb varicose veins, and chronic tonsillitis were statistically significantly more common (p < 0.05). The UCTD patients exhibited comorbidities and involvement of at least three body systems, whereas among patients without UCTD, somatic morbidity was limited to one or two clinical entities.
The cohort observational study determined the effect of UCTD on the incidence of miscarriage and preterm labor; thus, UCTD may be considered a risk factor for failure to carry a pregnancy to term. With UCTD, the risk of failure to carry a pregnancy to term increases by 3.4 times. During the observation period, the incidence of new cases of miscarriage and preterm labor amounted to 18.6 %. In this connection, it is reasonable to screen patients for UCTD at the stage of preconception preparation in order to promptly treat UCTD and improve pregnancy outcomes.
1. Ministry of Health of the Republic of Belarus; Belarusian Scientific Society of Cardiologists; Belarusian State Medical University. Diagnosis and treatment of hereditary and multifactorial connective tissue diseases. National clinical recommendations. Minsk, 2014.
2. Ibid.
3. Ministry of Health of the Republic of Belarus; Belarusian Scientific Society of Cardiologists; Belarusian State Medical University. Diagnosis and treatment of hereditary and multifactorial connective tissue diseases. National clinical recommendations. Minsk, 2014.
4. Ministry of Health of the Republic of Belarus. Resolution No. 17 of February 19, 2018 On approval of the clinical protocol “Medical Supervision and Provision of Medical Care to Women in Obstetrics and Gynecology.”
Available: https://formed.by/public/clinical_protocols/protocol_akusherstvo/КП_Медицинское_наблюдение_и_оказание_медицинской_помощи_женщинам_
в_акушерстве_и_гинекологии_пост_МЗ_19.02.2018_№_17.pdf
5. Ibid.
6. Ministry of Health of the Republic of Belarus; Belarusian Scientific Society of Cardiologists; Belarusian State Medical University. Diagnosis and treatment of hereditary and multifactorial connective tissue diseases. National clinical recommendations. Minsk, 2014.
7. Ministry of Health of the Republic of Belarus; Belarusian Scientific Society of Cardiologists; Belarusian State Medical University. Diagnosis and treatment of hereditary and multifactorial connective tissue diseases. National clinical recommendations. Minsk, 2014.
1. Ji ML, Jia J. Correlations of TIMP2 and TIMP3 gene polymorphisms with primary open-angle glaucoma. Eur Rev Med Pharmacol Sci. 2019;23(13):5542–5547. https://doi.org/10.26355/eurrev_201907_18287
2. Undifferentiated connective tissue dysplasia (the project of guidelines). Therapy. 2019;33(7):9–42 (In Russ.). https://doi.org/10.18565/therapy.2019.7.9-42
3. Fadeeva TS. Displaziya soedinitel`noj tkani: novy`e gorizonty` prob‑ lemy` [Connective tissue dysplasia: new horizons of the problem]. Cheboksary: Publishing House “Sreda”; 2018. 76 p. https://doi.org/10.31483/a-52
4. Il’ina IYu, Chikisheva AA. Course of the pregnancy in women with connective tissue disorders. Russian Journal of Woman and Child Health. 2020;3(3):182–188 (In Russ.). https://doi.org/10.32364/26188430-2020-3-3-182-188
5. Shestakova OV, Tetelyutina FK. The effectiveness of pregravidar preparation in women with infertility against the background of undifferentiated connective tissue dysplasia: a clinical case. Obstetrics and Gynecology: News, Opinions, Training. 2023;11 (2):57–63 (In Russ.). https://doi.org/10.33029/2303-9698-2023-11-2-57-63
6. Smetanin MYu, Pimenov LT, Chernyshova TE, Kononova NYu. Assessment of vitamin d in women of reproductive age with connective tissue dysplasia. Therapy. 2019;7:81–83 (In Russ.). https://doi.org/10.18565/ therapy.2019.7.81-83
7. Smirnova TL, Gerasimova LI, Sidorov AE, Chernyshov VV, Gubanova EA. Features of the course of pregnancy and childbirth in women with syndrome of undifferentiated connective tissue dysplasia. Practical Medicine. 2018;16(6):39–44 (In Russ.). https://doi.org/10.32000/20721757-2018-16-6-39-44
8. Novikova SV, Dalnikovskaya LA, Budykina TS, Biryukova NV, Klimova IV. Diagnostic and prognostic value of the study of biochemical markers of the threat of abortion in women with a short cervix. Russian Bulletin of Obstetrician-Gynecologist. 2020;20(4):18–26 (In Russ.). https://doi.org/10.17116/rosakush20202004118
9. Shestakova OV, Tetelyutina FK. Health status of married couples with infertility on the background of undifferentiated connective tissue dysplasia. Russian Journal of Human Reproduction. 2018;24(4):41–47 (In Russ.). https://doi.org/10.17116/repro20182404141
10. Druk IV, Nechaeva GI, Rezinovskaya TL. Deficiency of body mass in a group of young-age patients with connective tissue dysplasia. Thera‑ py. 2020 Sep 22;6_2020:52–58 (In Russ.). https://doi.org/10.18565/therapy.2020.6.52-58
11. Rozhkova M. Yu., Nechaeva G. I., Lyalukova E. A., Kulikova O. M. Variants of acid-breasting function of the stomach in patients with connective tissue dysplasia. Experimental and Clinical Gastroenterolo‑ gy. 2018;158(10):80–85 (In Russ.). https://doi.org/10.31146/1682-8658ecg-158-10-80-85
12. Kytko O.V., Dydykina I.S., Sankova M.V., Kryuchko P.V., Chilikov V.V. Pathogenetic aspects of magnesium deficiency in connective tissue dysplasia syndrome. Problems of Nutrition. 2020;89(5):35–43 (In Russ.). https://doi.org/10.24411/0042-8833-2020-10064
13. Seryogina DS, Nikolayenkov IP, Kuzminykh TU. Obesity represents a strong pathogenetic link with the pathology of pregnancy and childbirth. Journal of Obstetrics and Women’s Diseases. 2020;69(2):73–82 (In Russ.). https://doi.org/10.17816/JOWD69273-82
14. Andreeva EN, Sheremetyeva EV, Fursenko VA. Obesity — threat to the reproductive potential of Russia. Obesity and metabolism. 2019;16(3):20–28 (In Russ.). https://doi.org/10.14341/omet10340
15. Pestrikova TIu, Knyazeva TP. Irregularities during pregnancy progression and childbirth in women with a low body weight. Russian Bulletin of Obstetrician-Gynecologist. 2019;19(3):63–69 (In Russ.). https://doi.org/10.17116/rosakush20191903163
16. Ivanova II, Makarova II, Ibragimova ShM, Saidalieva KD, Sultonova FS. Structural and functional features of the erythroid germ in patients with connective tissue dysplasia. Ural Medical Journal. 2022;21(6):136–143 (In Russ.). https://doi.org/10.52420/2071-5943-2022-21-6-136-143
17. Delyagin VM, Aksyonova NS, Rumyantsev SA. Uterine Bleeding in Adolescents with Heritable Connective Tissue Disorders. Effective Pharmacotherapy. 2021;17(41):8–11 (In Russ.). https://doi.org/10.33978/2307-3586-2021-17-41-8-11
18. Anikin VV, Beganskaya NS, Andreeva EV, Izvarina OA, Nikolaeva TO, Gromnatsky NI. Features of peripheral blood at a dysplasia of connective tissue. Kursk Scientific and Practical Bulletin “Man and His Health”. 2019;4:14–20 (In Russ.). https://doi.org/10.21626/10.21626/vestnik/2019-4/02.
19. Proshin AN, Mashin VV, Belova LA, Belov DV. Structure of intracranial veins and elastic-viscous properties of red blood cell membranes in adolescents with connective tissue dysplasia. Ul’yanovskiy Mediko-biologicheskiy Zhurnal. 2021;3:47–60 (In Russ.). https://doi.org/10.34014/2227-1848-2021-3-47-60
20. Sukhikh GT, Prilepskaya VG, Aganezova NV, Andreeva EN, Baranov II, Dolgushina NV, Zarochentseva NV, Karakhalis LYu, Katkova NYu, Kepsha MA, Mezhevitinova EA, Nazarenko EG, Nazarova NM, Podzolkova NM, Smetnik AA, Tapilskaya NI, Uvarova EV, Hamoshina MB, Chernukha GE, Yakushevskaya OV, Dzhenina OV, Yarmolinskaya MI. National medical eligibility criteria for contraceptive use 2023: review. Bulletin of Reproductive Health. 2024;3(1):9–67 (In Russ.). https://doi.org/10.14341/brh12705
21. Novitskaya TV, Yahorova TY, Vakulchyk VG. Comparative assessment of the course and outcomes of pregnancy in patients with undifferentiated connective tissue dysplasia using conventional and personalized preconception preparation. Journal of the Grodno State Medical Uni‑ versity. 2023;21(2):161–166 (In Russ.). https://doi.org/10.25298/22218785-2023-21-2-161-166
22. Studennikova VV, Severgina LO, Dziundzia AN, Korovin IA. Lower extremity varicose veins in childhood and at a young age: Mechanism of development and specific features. Russian Journal of Archive of Pathology. 2017;79(4):56–60 (In Russ.). https://doi.org/10.17116/patol201779456-60
23. Fadeeva TS, Molokanova MV, Pavlov OG. The influence of the severity of undifferentiated connective tissue dysplasia on pregnancy. Journal of New Medical Technologies. 2019;3;12–17 (In Russ.). https://doi.org/10.24411/2075-4094-2019-16395
24. Kalaeva GYu, Khokhlova OI, Deev IA, Мikheenko GA. Risk factors associated with the development of undifferentiated connective tissue dysplasia. Bulletin of Siberian Medicine. 2018;17(2):41–48 (In Russ.). https://doi.org/10.20538/1682-0363-2018-2-41-48
Elena N. Grudnitskaya — Cand. Sci. (Med.), Assoc. Prof., Department of Obstetrics and Gynecology
P. Brovki str., 3, bldg. 3, Minsk 220013
Larysa М. Nebyshynets — Cand. Sci. (Med.), Assoc. Prof., Head of the Department of Obstetrics and Gynecology
P. Brovki str., 3, bldg. 3, Minsk 220013
Grudnitskaya E.N., Nebyshynets L.M. Pregnancy outcomes in patients with undifferentiated connective tissue disease: An observational cohort prospective study. Kuban Scientific Medical Bulletin. 2024;31(4):17-29. https://doi.org/10.25207/1608-6228-2024-31-4-17-29
Sedin str. 4, Krasnodar, Russian Federation, 350063
Tel.: (861) 268 55 02
E-mail: kubmedvestnik@ksma.ru, kubmedvestnik@mail.ru




































